

Wake Up, America! Jeffrey Rose and the Case for Sleep as MAHA Policy
By Amy Sapola, PharmD, Contributor, The MAHA Report
In Ohio, the bus arrives at 6:50 a.m., before the winter sun has fully risen. I know this because I regularly do what many parents do each weekday. I walk into a dark bedroom and say, “Wake up, it’s time for school.”

What happens next is so routine we rarely stop to question it. A teenager gets out of bed while their body still needs sleep. Within minutes, the stress response starts. Cortisol rises as they rush to get dressed, grab something to eat, and hurry to the bus stop or get in the car. The school day begins before their brain and body have fully woken up. This leaves many adolescents trying to learn, focus, and perform while they are still physically exhausted.
The science is increasingly clear: this routine is not benign. It may be one of the most widespread and under-recognized health stressors affecting American adolescents.
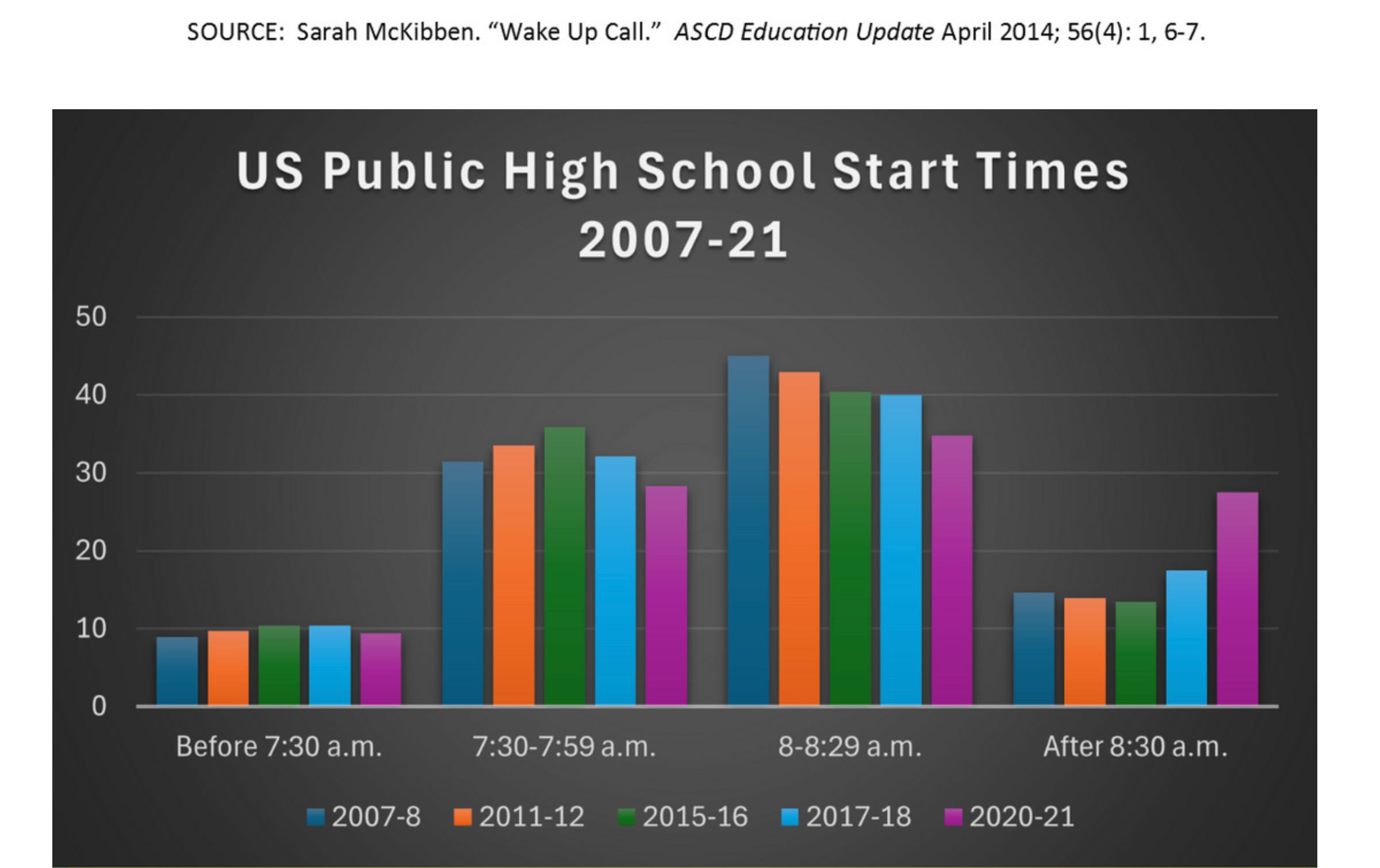
The 2025 Make America Healthy Again Commission Report identifies insufficient sleep among children and adolescents as part of a growing national health crisis. Structural factors play a major role: 43% of U.S. public high schools start before 8:00 a.m., and roughly one in three teenagers reports falling asleep during class.
The broader data make the implications difficult to ignore:
Nearly four out of five U.S. high school students sleep fewer than eight hours on school nights, according to the CDC’s Youth Risk Behavior Survey, despite recommendations that teenagers get 8–10 hours of sleep per night.
Students who sleep fewer than 8 hours are significantly more likely to report difficulty concentrating, lower grades, and higher rates of absenteeism.
Approximately 7 million American children (11.4%) ages 3–17 have been diagnosed with Attention-Deficit/Hyperactivity Disorder, with prevalence rising to 18–20% of boys and 8–10% of girls ages 12–17.
More than 40% of high school students report persistent feelings of sadness or hopelessness, and nearly one in five have seriously considered suicide, according to CDC data. Sleep plays a central role in mental health because it regulates neural circuits involved in mood, stress response, and emotional processing. Chronic sleep deprivation is strongly associated with increased risk of anxiety, depression, and impaired emotional resilience.
About 21% of U.S. adolescents have obesity, and short sleep duration has been linked in the medical literature to higher BMI, insulin resistance, and increased cardiometabolic risk.
Sleep also plays a key role in immune system health. When teenagers are sleep deprived, their bodies are less able to fight off infections and recover quickly. In crowded school environments—where colds and flu spread easily—this matters: illness is the leading cause of school absenteeism in the U.S., responsible for millions of missed school days each year, and research shows that people who sleep fewer than six hours are about four times more likely to develop a cold after exposure.
Taken together, these trends highlight what the MAHA Commission emphasizes: adolescent sleep is not merely a lifestyle issue. It is a structural health determinant shaped by policy decisions, with consequences for the cognitive, emotional, and physical well-being of an entire generation.

The Next Public Health Reform: Sleep
Jeffrey Rose did not set out to become a sleep advocate. Trained in nutrition and psychology at New York University, he spent decades working in behavior change—studying hypnosis, coaching people through addiction recovery, and helping clients improve diet and lifestyle habits. Over time, however, one pattern kept emerging in his work: when sleep was disrupted, every other intervention became less effective.
With client after client, Rose noticed that poor sleep undermined the very behaviors people were trying to improve. Appetite regulation faltered, impulse control weakened, mood became unstable, attention declined, and even the best health plans were difficult to maintain.
“Sleep kept showing up,” Rose told me. “When people aren’t sleeping well, impulse control gets harder, mood gets unstable, attention drops, and even sticking to healthy habits becomes much more difficult.”
Those observations led Rose to a conclusion that sits at the heart of this story: the next major public health reform may not involve a new drug, supplement, or technology. It may simply involve letting people—especially teenagers—sleep.
That idea sits at the center of the movement led by Start School Later, which works to align school schedules with adolescent biology. The organization’s advocacy is grounded in decades of sleep research showing that puberty naturally shifts the circadian rhythm later.
In practical terms, many teenagers do not naturally feel sleepy until around 11 p.m., making it nearly impossible to get the 8–10 hours of sleep experts recommend if school begins before 8:30 a.m.
Recognizing this mismatch, the American Academy of Pediatrics issued a landmark recommendation in 2014, urging middle and high schools to start no earlier than 8:30 a.m. In 2015, the CDC echoed the guidance, citing evidence that later start times are associated with improved sleep duration, mood, and academic outcomes. In 2017, the American Medical Association and in 2018, the American Academy of Sleep Medicine both endorsed starting school later.
Yet despite the science, early schedules remain common across the United States.
Rose believes that disconnect has real consequences.
“We’re building a system where teenagers are chronically sleep deprived,” he said. “And then we wonder why attention problems, anxiety, and burnout keep increasing.”
When communities do shift schedules, the results can be striking. A three-year multi-state study led by Kyla Wahlstrom et. al. found that delaying school start times by 25–60 minutes increased weeknight sleep by roughly 30–60 minutes and was associated with improvements in daytime alertness, mood, attendance, and reduced caffeine use. One finding in particular stood out to me as a parent: when a high school moved its start time from 7:35 a.m. to 8:55 a.m., car crashes among teen drivers aged 16–18 fell by about 70 percent.
Why the System Matters More Than Sleep Hygiene Alone
As a clinician, I value sleep hygiene. Rose does too. He talks about reducing evening light exposure, limiting caffeine (especially in the afternoon), avoiding heavy late meals, and regular daily movement. He also points out that there is no doubt that alcohol is a disruptor of sleep architecture. These are useful, practical levers.
But Rose’s point is that we cannot “sleep hygiene” our way out of a structurally sleep-deprived system.
During our interview, Rose said something that felt almost too obvious to be controversial: we would never wake a sleeping baby and call it discipline. Yet we do it to adolescents during their most intense period of neurodevelopment and then act surprised when mood, motivation, and focus suffer.
Sleep and ADHD
Rose emphasized a factor that is often minimized in discussions about attention and behavior: chronic sleep deprivation. Research consistently shows that adolescents who sleep fewer than the recommended 8–10 hours per night and adults who routinely sleep fewer than 7 hours per night demonstrate measurable impairments in attention, executive function, impulse control, mood regulation, and working memory. Even modest but sustained sleep restriction (losing roughly an hour per night) can produce cognitive effects that resemble or amplify symptoms associated with ADHD.
As Rose stated during our interview, “When you chronically deprive the brain of sleep, you’re not just making someone tired, you’re changing how that brain functions.” His argument is not that sleep explains all attention problems, but that it is a foundational variable that deserves evaluation before diagnostic labels are assigned.
National data underscore why this matters. According to the CDC’s 2022 National Survey of Children’s Health, approximately 11.4% of U.S. children aged 3–17 (about 7 million) have never been diagnosed with ADHD. Among adolescents ages 12–17, prevalence is higher: roughly 18–20% of boys and 8–10% of girls have ever received a diagnosis.
Rose reflected on those figures: “We’re seeing more and more young people labeled with attention disorders. Before we assume this is purely a psychiatric issue, we have to ask what else is happening in their environment and in their bodies.”
At the same time, stimulant prescribing has increased. Analyses of national prescription and controlled-substance distribution data show that total prescription stimulant volume in the U.S. approximately doubled between 2006 and 2016, with continued growth in the years since, particularly among adolescents and adult women.
Rising diagnosis and prescribing rates can reflect multiple factors: broader screening, changes in diagnostic criteria, improved access to care, school performance pressures, reduced stigma, etc. Sleep deprivation is unlikely to be the sole driver, but it is one of the few modifiable physiologic variables that directly affect attention, and we can influence it through policy.
The Connection Between Addiction and Sleep
Rose drew a stark comparison during our interview, warning that we are normalizing patterns in adolescents that closely resemble a cycle of dependency. “We’re training kids for addiction with hangovers,” he said, referring to the pattern of chronic sleep deprivation followed by attempts to override fatigue with stimulants, whether caffeine, energy drinks, or prescription medications.
When teenagers are routinely exhausted, then taught to chemically compensate rather than correct the underlying sleep deficit, we reinforce a physiology of depletion and artificial recovery. His concern was not about appropriate medical use when truly indicated, but about a broader cultural pattern: creating the deficit first, then medicating the consequence without addressing the root cause.

Jeffrey Rose with his teenage daughter, Rebecca
The Takeaway
Rose’s message to the MAHA community is clear: treat sleep as essential, not an indulgence. Adequate sleep supports attention, emotional regulation, metabolic stability, immune function, and long-term cardiometabolic health. It sits upstream of nutrition, mental health, learning, and resilience. When sleep suffers, every other intervention—diet, exercise, medication, even therapy—becomes less effective.
For parents, the lesson begins at home. Children learn what “normal” looks like by watching us. If we model late nights, constant exhaustion, and a culture that glorifies busyness over recovery, they continue that pattern. But when families protect sleep by setting consistent routines, limiting late-night screens, dimming evening lights, and valuing rest as much as productivity, we teach something far more valuable: sleep is foundational to every aspect of health.
If we normalize chronic exhaustion in adolescence, early start times, late-night devices, and relentless performance pressure, we should not be surprised when those same individuals reach adulthood depleted, hormonally and metabolically dysregulated, and searching for ways to compensate for years of lost recovery. Burnout rarely begins in midlife.
The science already points toward solutions. The American Academy of Pediatrics recommends that middle and high schools start no earlier than 8:30 a.m., recognizing that adolescent circadian rhythms naturally shift later during puberty. Aligning school schedules with biology is not indulgence – it is evidence-based prevention.
For parents who want to advocate for change in their local school district, the nonprofit Start School Later provides research, policy guidance, and practical tools to help communities shift school schedules.
Amy! Pleasure to meet another PharmD on the right side of history! Sleep is critically important for both physical and mental aspects. Totally agree and should be prioritized!
You may appreciate my piece here on ADHD and how that changed my view of the profession. These are hard core medications and should not be prescribed, especially to children: https://unorthodoxy.substack.com/p/adhd-and-me-how-the-narrative-broke
As a parent of two post-teens, later school start times means waking up later. Yes. True. It also means going to bed later for most teens. Early or late school start times are meaningless. It's the amount of sleep, not the time one gets up. Unless PARENTS enforce a bed time, nothing schools do will make one bit of difference.